Publication: Institute of Medicine (2005), Making Better Drugs for Children with Cancer. Peter Adamson, Susan Wein, Joseph Simone and Hellen Gellband. 57 pages. peer reviewed.
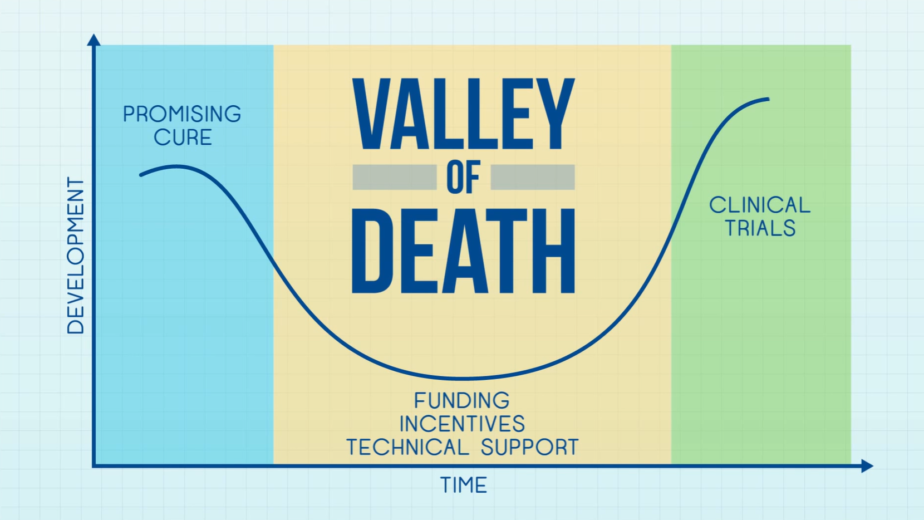
Summary: This report cites a then near-absence of research in pediatric cancer drug discovery. Over the preceding 40 years before the report, childhood cancer in countries like the United States had shifted from being largely fatal to having high long-term survival rates, thanks to intensive use of drugs originally developed for adults. However, further progress now requires new, targeted treatments because simply intensifying existing therapies yields only modest gains and significant side effects. Despite promising molecular discoveries that could lead to more precise drugs, pharmaceutical companies had had little financial incentive to invest in pediatric cancer research due to the small market size. Organizations such as the National Cancer Institute (where technical capacity for drug discovery and development for pediatric cancers already exists), and the Food and Drug Administration were thought to be need to reduce delays in starting pediatric clinical trials if one wants to see better outcomes in terms of curing cancer in children. The takehome was that “public-private partnership” could knit together the pieces in a virtual research and development (R&D) network.
Recommendation 1: A new public–private partnership, involving government, industry, academic and other research institutions, advocacy groups, philanthropies, and others, should be formed to lead pediatric cancer drug discovery and development.
Recommendation 2: The National Cancer Institute should assume responsibility as the developer of last resort for agents that show promise only in children if companies decide not to proceed with full-scale development.
Recommendation 3: The pharmaceutical industry, National Cancer Institute, and Food and Drug Administration should act to reduce the delay in beginning pediatric clinical studies of agents in development for adult cancers.
Perspective: One can directly measure the effectiveness of each recommendation.
Recommendation 1: The NIH (NCI) in partnerships with universities has since assumed a role in testing existing (adult cancer) drugs effectiveness for childhood cancer in cell line models systems and mice via the PIVOT program, which relies to a great extent on what drugs are deposited by pharma companies in the NCI CTEP Portfolio. From drugs studied by PIVOT, zero have reached an FDA approval for a childhood cancer tested (the approval attesting to the effectiveness of the medicine). Parenthetically, Selumetinib reached secondary FDA approval in pediatric NF1-related neurofibroma tumors, but these were not studied by PIVOT.
NIH NCATS has the capacity for discovering new drugs at scale for specific pediatric cancers, and has done so on occasion. However, no single government agency we are aware of intentionally and systematically develops new treatments for childhood cancers from scratch. Pharma does, sometimes with the help of cooperative groups (see COG below). Since 2005, 9 drugs have been intentionally developed for childhood cancer as a primary indication and first FDA approval (generally involving a pharma company, and possibly the COG cooperative trial group).
Recommendation 2: The NCI facilitated the revival of a discontinued drug, ganitumab, for a clinical trial by the Children’s Oncology Group (COG, who are often sponsored by NCI funding). Ganitumab had no clear benefit for patients.
Recommendation 3: This recommendation speaks to increasing the throughput of adult cancer drugs for a secondary use in children. Since 2005, at least 18 adult cancer drugs have reached FDA secondary approval for childhood cancer. Meanwhile, the intention to develop a childhood cancer drug from scratch is now motivated by the Pediatric Priority Review Voucher, a legislated FDA financial incentive for new molecular entities (brand new medicines) for childhood cancer.
Overall, since 1978 only 14 new medicines exist for childhood cancer – yet 1 in 5 children will not be cured. As federal funding for childhood cancer drug development becomes less certain, we favor the pharma-led efforts for bespoke childhood cancer medicines that led to those 9 approvals since 2005. However, a strategy to include adult markets that are profitable with the same pediatric cancer medicines could be necessary to finance and sustain production of these needed drugs.