

Diabetes GPL-1 Agents and the Muscle-loss Problem
Type II Diabetes treatment and prevention are a pressing worldwide medical and sociological indication, driving $966 billion in healthcare expenses annually worldwide in a trend that is only increasing. The market is therefore amenable to a wide range of treatments and treatment combinations
DIABETES AND MUSCLE-LOSS
FOXO1 and diabetes
Diabetes may be the largest and fastest growing biomedical research market (CAGR 34.6%) . FOXO1 has been well-studied as a factor in Type II Diabetes and found to have tissue-specific and physiologically-dependent roles. The simplest approach for a FOXO1 related therapeutic would be to deliver a FOXO1 bioPROTAC (protein degrader) to skeletal muscle specifically. In glucose homeostasis, skeletal muscle acts as the body’s primary glucose sink (taking up approximately 75-80% of glucose after meals), burning glucose for energy, or storing glucose as glycogen.
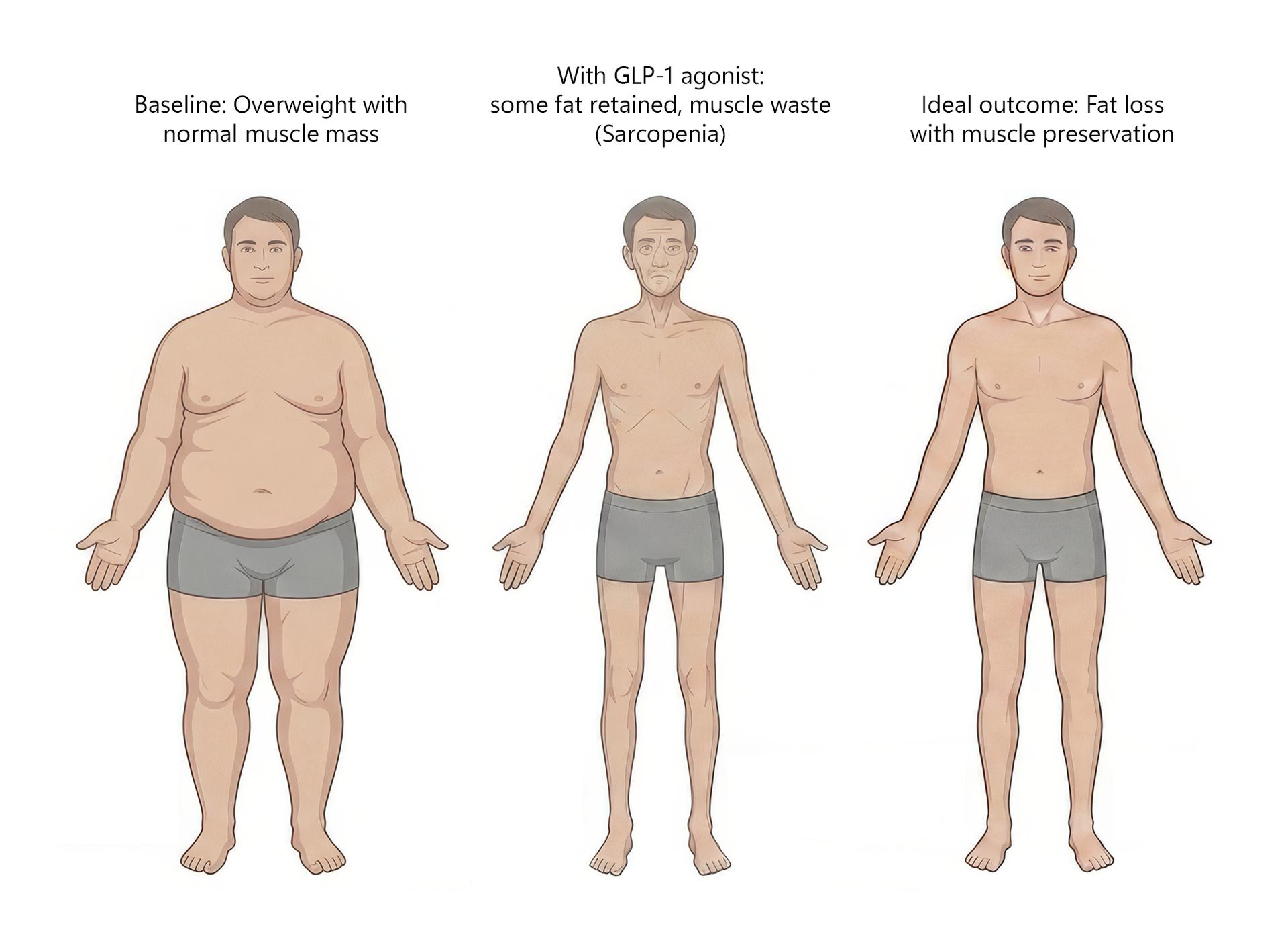
Based upon genetic proof-of-concept studies, a FOXO1 bioPROTAC degrader would increase glucose uptake and oxidation, reduce lipid uptake and oxidation, and decrease muscle atrophy. Co-administration of GLP-1 receptor agonists and a FOXO1 bioPROTAC degrader would be an interesting avenue to explore, given that rapid weight loss with GLP-1 receptor agonists can result in loss of lean muscle mass (sarcopenia).
Given that FOXO1 mediates pathways of muscle breakdown (atrophy, catabolism, muscle growth inhibition), a significant net positive protein balance and a muscle mass increase could occur with combined GLP-1 receptor agonist and FOXO1 bioPROTAC degrader treatment. Tissue-specific delivery to skeletal muscle is now possible given preclinical advances in muscle-specific lipid nanoparticles and clinical advances in safe & effective intravenous administration of mRNA therapeutics delivered by lipid nanoparticles.